
In North Carolina, where a clinician practices can make all the difference for someone seeking maternity care — it’s the birth equivalent of “location, location, location.”
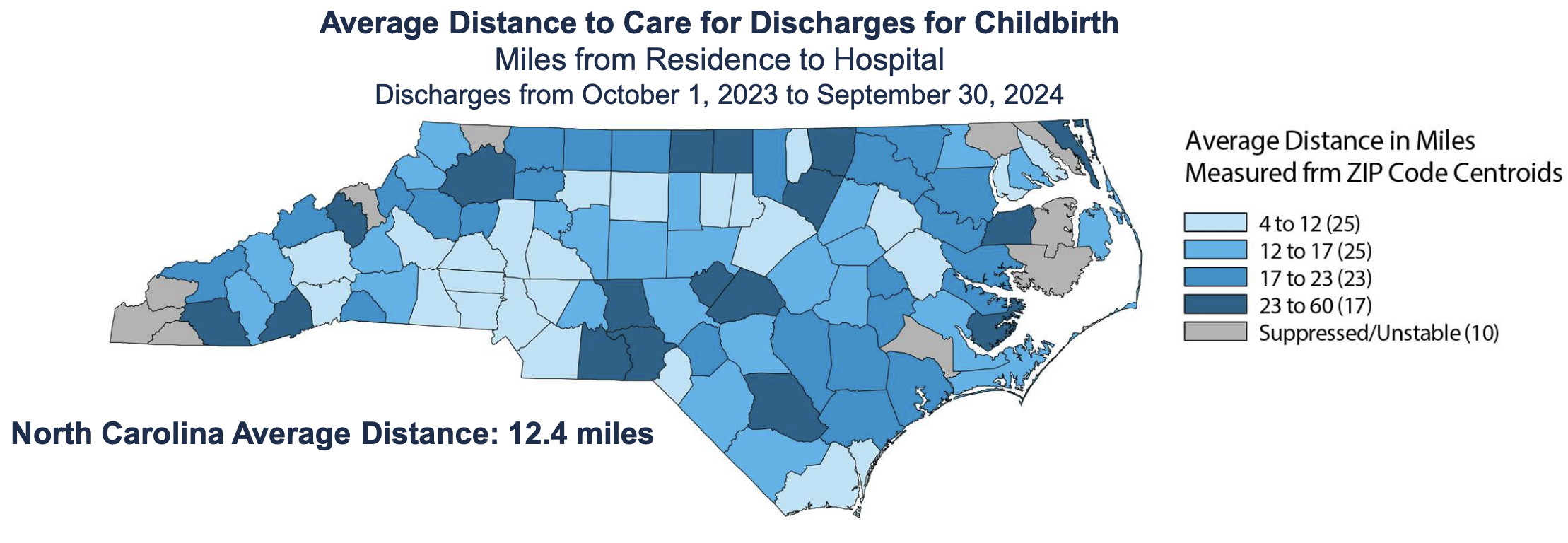
Dozens of counties have no local obstetrics care, so families are forced to travel long distances for deliveries. That distance to care for rural patients has been linked to higher rates of cesarean sections, preterm births and maternal complications.
And the state struggles with maternal and infant health outcomes; it received a D+ in the 2025 report card from the March of the Dimes. North Carolina has the 11th highest infant mortality rate in the United States.
The challenge to getting maternal and infant care isn’t necessarily a shortage of providers, lawmakers learned last Tuesday during a presentation at a legislative committee hearing.
“This is not a supply issue. This is a distribution issue,” said Erin Fraher of the Sheps Center for Health Services Research at UNC Chapel Hill. “We do not have people where we need them.”
More clinicians, uneven access
The good news is that from 2005 to 2024, the number of physicians providing obstetric deliveries in North Carolina ticked up slightly, even as the number of births remained flat, according to state data.
“If you view this as a workload measure, we actually have fewer births per physician,” Fraher told lawmakers at the Joint Legislative Oversight Committee on Health and Human Services.
The state’s maternity workforce also includes certified nurse midwives, who attended about 16 percent of births in 2024, compared with the 81 percent of deliveries by physicians, according to the Sheps Center data.
The General Assembly also passed a bill in 2023 that allowed experienced certified nurse midwives to practice without physician supervision if they had completed at least 24 months and 4,000 hours of clinical practice. (The same bill also tightened North Carolina’s restrictions on abortion.) The change to rules governing midwifery was intended to expand access to maternity care in underserved areas. Advocates, at the time, had hoped that it would be “the tip of the iceberg” for similar policy.
The number of certified nurse midwives the year the legislation passed was 425, with 392 of those being in a collaborative practice. Since then, the number has grown to 501 — and just over half (257) are practicing independently.
As the maternity workforce has grown, so has the number of standalone birth centers. Previously, the state had only one standalone birth center where certified nurse midwives, under the supervision of a physician, provided maternal and infant care. Five more centers have opened since 2023.
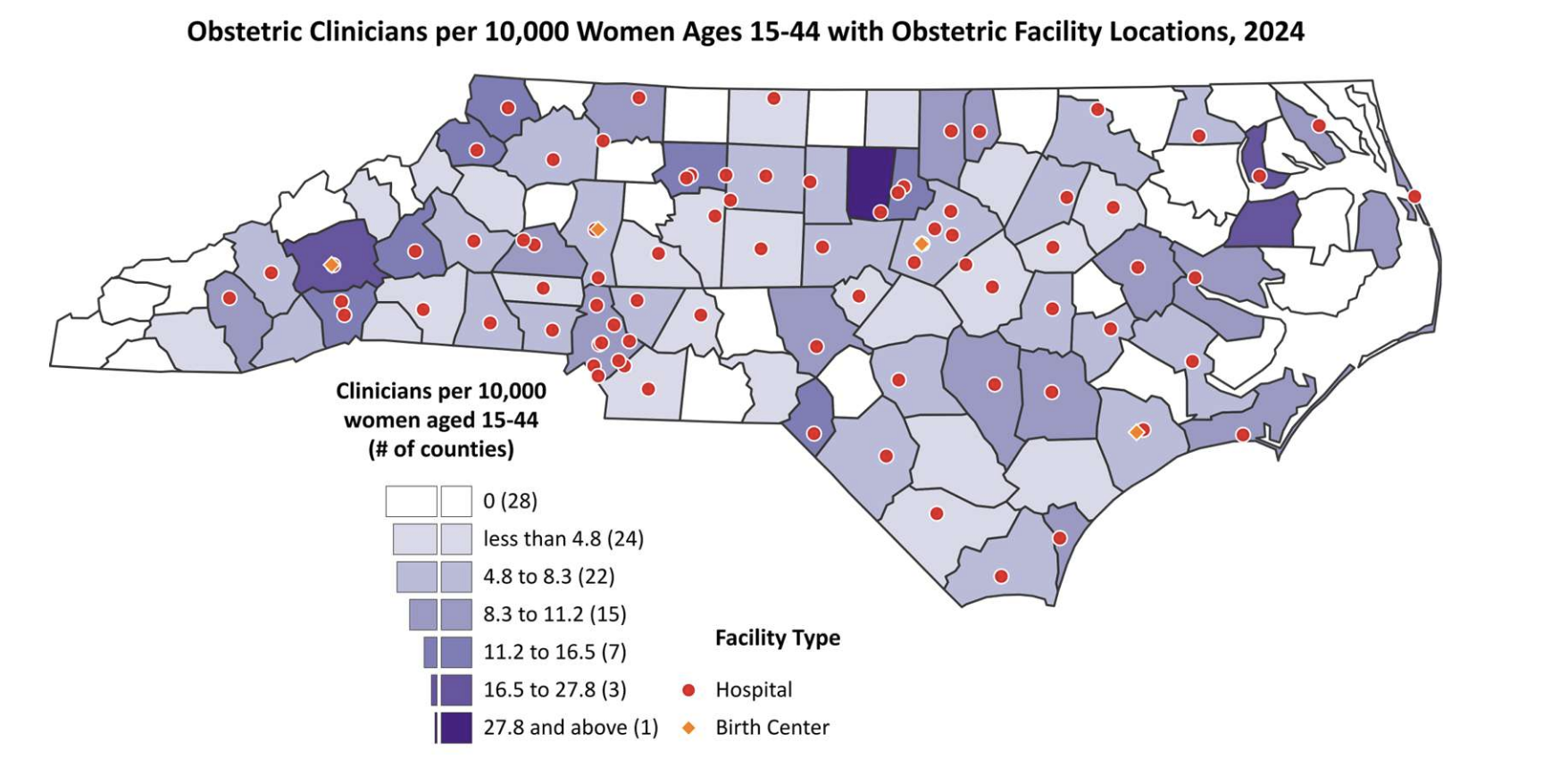
Even so, combined data about physicians and certified nurse midwives reveal that there are 28 counties with no clinicians or facilities providing deliveries. The longest distances to care were observed in 17 counties, with distances between 23 and 60 miles. In mountain counties, that can take more than an hour to traverse.
The geography of maternity care
The majority of clinicians appear to work in urban areas, according to state data. Only 13.4 percent of physicians providing obstetric care work in rural areas. Just 17.3 percent of collaborative certified midwives do, and 11.7 percent of independent certified nurse midwives.
“We have seen in many states this regression of distribution,” said Rep. Grant Campbell (R-Kannapolis), a longtime OB-GYN. “Even if they begin in underserved areas when that independent practice is granted, we see a migration to the same distribution of physicians.”
Fraher pointed to a number of factors that might be contributing to that.
“One of the things we’re very conscious of is you can only work in a county where there’s a facility to hire you. There has to be a facility, and there has to be a facility that’s willing to hire you,” she answered. “I’m wondering whether there’s also some inertia that’s happening in terms of hospitals not having been in the past employing independent [certified nurse midwives].”
That lack of facilities is a growing problem; the Sheps Center estimates that between 12 and 18 rural hospitals have closed.
In 2024, nearly 12,000 births originated from those counties “where presumably if there were a hospital or birth center, somebody would have chosen to deliver locally,” Fraher added.
Recent closures were top of mind for Sen. Jim Burgin (R-Angier), who represents two of the 17 counties with the longest travel times.
“About two years ago, our hospital closed all the OB services, “ he said. “There were 435 children born the year before it was closed, and it’s just amazing to me that we have almost a third of our counties that don’t have OB services and delivery.”
That can directly affect outcomes for mother and infant, according to a study mapping maternal care deserts performed by researchers from Appalachian State and NC State universities. The study found that in North Carolina, travel times and distances to clinical care were associated with higher cesarean delivery rates, more severe maternal morbidity, preterm birth and higher rates of gestational diabetes.
“I'm very concerned about the high infant mortality rate as a mother who experienced three high-risk pregnancies,” said Rep. Ya Liu (D-Cary). “I know how hard, how challenging it can be for a family. And what are the solutions? What can we do?”
Fraher said improving outcomes often requires addressing issues beyond pregnancy care, including access to primary care and social factors affecting health.
Looking ahead
Campbell embraced the opportunity to highlight again the loss of a statewide initiative focused on improving maternal and infant health outcomes to his colleagues.
The Perinatal Quality Collaborative of North Carolina, which coordinated hospital teams working to improve care for mothers and newborns, began winding down operations last year after losing its roughly $905,000 annual budget tied to Medicaid funding.
The program had operated in dozens of hospitals statewide since 2009.
Campbell said the initiative had been “incredibly inexpensive” and had improved maternal and infant health outcomes.
Fraher said policymakers may also want to consider expanding graduate medical education programs that train obstetricians and family physicians in maternity care, since physicians often stay in the communities where they complete residency training.
While the number of providers continues to grow statewide, she said the core challenge remains ensuring that those clinicians practice where families need them most.
“The fundamental issue,” Fraher told lawmakers, “is distribution.”
This article first appeared on North Carolina Health News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.